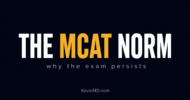
What does a modern internal medicine intern do all day (and night)? It turns out they spend 40% of their time at work using a computer, another 20% on other aspects of patient care that is not in the presence of the patient, 15% in educational activities, 5% on basic needs like walking around and eating, and only 12% in direct patient care. Direct patient care includes interviewing patients, examining patients, doing procedures for patients, talking to family members, and all activities that are in the direct presence of the patient or their family.
This information is reviewed in the recent NEJM Journal Watch which discusses an Annals of Internal Medicine article about a 2012 observational project that used trained observers to look at what interns actually do with their time. They spend 60% of their time in “indirect patient care” which includes discussion of cases with other providers and making chart notes. Unfortunately most of this time sounds like it is largely documentation of the 12% of the time they actually take care of patients. Two-thirds of the indirect patient care time, or 40% of their total work time, was spent on computers, mostly in computer generated documentation of care.

Graph depicting how internal medicine interns spent their time in 2012
Use of computers is intended to improve patient care. In many ways it may improve patient care by making information more easily available, allowing for care reminders, protocols, etc. to assist in care.
Arguing against this is the fact that a similar study noted in this NEJM article showed that in 1989 interns spent 20% of their work day in direct patient care. Keep in mind that their work day was much longer in those days before mandatory limitations on house staff work hours, so the absolute time spent on direct patient care was probably even greater than this percentage difference suggests. This reduction in relative and actual time in direct patient care does not portend well for training of young physicians. If interns spend nearly 40% less of their time interviewing, counseling, examining and doing thing to/with patients than physicians did 20+ years earlier it seems unlikely that they will develop better patient care skills.
This is not incongruent with my observations of how medical care is going in general. We are spending more and more time in the arena of “indirect patient care.” This is a euphemism for making chart notes, completing tasks required by various outside parties. Insurance companies want documentation for physicians get reimbursed, they also demand information and documentation to get prior authorizations for everything from medications and testing to surgery. Others who need physicians to provide documentation include employers, nursing homes, schools, hospitals, coaches, parents, children, department of transportation officials, pharmacies, and attorneys among others. It seems like I spend many hours daily on tasks that provide little or no direct health benefits to my patients. This study suggests to me that we are indoctrinating young physicians into this mindset early.
The article ends with, “However, things clearly are moving in the wrong direction. These fascinating data ring completely true and should give program directors impetus to reevaluate critically the present routines of clinical training.”
I could not agree more. The issue though is not just in how physicians are trained. It is in what the system we work within demands from physicians in terms of documentation.
Edward Pullen is a family physician who blogs at DrPullen.com.